

Shoulder instability
These are recurrent shoulder dislocations. Shoulder mobility is very important, but its stabilization system is more fragile than that of the hip, for example.
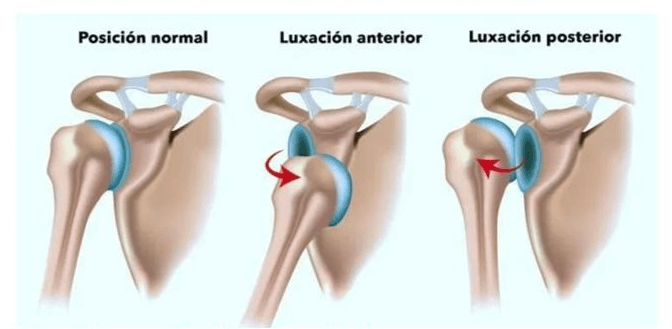
In other cases, instability is responsible for a purely painful shoulder. Instability is more frequently anterior and post-traumatic, and frequently affects young people.
Symptoms of shoulder instability
Instability is often painless or only mildly painful, except in cases of subluxation or dislocation. When pain is present, it is usually located in the anterior aspect of the shoulder.
It can present in 2 clinical forms:
Particular attention should be paid to patients with congenital hyperlaxity (external rotation greater than 90º with the elbow close to the trunk or the possibility of placing the thumb on the anterior surface of the forearm) for both diagnosis and therapeutic indication.
What complementary tests should be performed for shoulder instability?
X-rays are performed to investigate injuries to the humerus and scapula. This examination is insufficient to make a detailed diagnosis of the ligaments, tendons, glenoid rheodetum, and cartilage. An arthral scan will routinely be used to more accurately diagnose bone injuries and decide which surgical technique to use to stabilize the shoulder.
Treatments for shoulder instability
After a shoulder dislocation, a reduction is usually performed, which consists of repositioning the shoulder under general anesthesia. The treatment is not emergency surgery unless there is a labrum injury that prevents reduction of the dislocation.
The arm is then immobilized for three weeks with the arm held against the body in internal rotation to allow the capsule and ligaments to heal. After these three weeks, a retraining program begins to retrain the shoulder joint to work in a correct position, using muscle strengthening and proprioceptive exercises.
Despite this, the recurrence rate of dislocation is 30%. After two recognized episodes of dislocation or subluxation, a surgical solution is proposed.
The main stabilization options are the Latarjet procedure (coracoid block) and arthroscopic stabilization or Bankart procedure. The choice of surgical technique is based on clinical and radiological criteria.
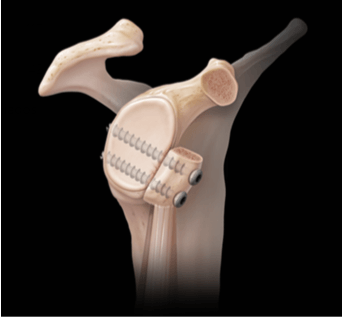
Coracoid block (Latarjet)
It is indicated for athletes and professionals who perform violent movements with a risk of tearing (rugby, judo, volleyball, basketball, etc.) or when there are significant injuries to the glenoid or humerus, provided there is no hypermobility.
The surgery is performed "open." A piece of bone is taken from the coracoid and attached to the anterior and inferior part of the glenoid. This procedure reinforces shoulder stability with additional bone and tendon support (the joint tendon of the biceps and coracobrachialis muscles). It prevents dislocation when the shoulder is abducted and externally rotated.
Arthroscopic stabilization or Bankart procedure
This procedure is indicated primarily for athletes without significant impact on the shoulder or in cases of moderate bone injury, provided there is no hypermobility.
It involves arthroscopic reattachment of the labrum and the inferior glenohumeral ligament. This procedure can be combined with filling the posterior notch using the infraspinatus tendon, which covers the area of the bone defect.

Modalities of hospitalization and re-education
The surgical procedures described above can be performed on an outpatient basis without hospitalization. Occasionally, depending on the patient's medical history, they may require a 24-hour hospital stay.
They are performed under double anesthesia. The arm is anesthetized for a prolonged effect (12 hours) to relieve postoperative pain. General anesthesia is also used for preoperative comfort.
After the procedure, an orthosis is placed to keep the arm attached to the trunk for 3 weeks for the coracoid block and 6 weeks for the Bankart block, to promote tissue healing.
Re-education begins early and continues until full mobility and strength are restored (3 to 5 months). This re-education with the physical therapist will be complemented with self-re-education exercises.
To resume physical activity and non-violent sports, wait approximately 3 months. For contact, mechanical, or combat sports, wait 6 months. These times are guidelines; follow your surgeon's instructions.
This information is provided by specialized healthcare personnel for informational purposes only and does not replace medical advice.
If you would like to make an appointment with our shoulder specialist in Bilbao, you can contact us by phone at 946 941 347 or by using the following form.